소화기학 21 — 하부위장관 출혈, 혈관질환 및 소장질환 학습노트
좌측 PDF 페이지와 1:1로 정렬되는 우측 노트. 본문은 통독용 해설, 우측 여백의 기출·암기는 곁눈질용 — 떠올린 뒤 해설을 펼치는 능동회상 방식입니다.
page1
하부위장관 출혈·혈관질환 및 소장질환 (강의 개요)
표지lower GI bleedingvascular diseasesmall bowel diseasecourse intro
경희의료원 소화기내과 오신주 교수님. 본 강의는 하부위장관 출혈(LGIB)을 중심으로 혈관질환(장 허혈)과 소장질환을 다룬다. 2026년부터 담당 교수가 바뀌어 수업 내용에서 출제될 가능성이 높아짐.
page2
LGIB 정의 및 해부학적 경계 (Ligament of Treitz)
정의/총론lower GI bleedingLigament of TreitzGI bleeding epidemiologycolon as main source
정의: Ligament of Treitz 하부에서 발생하는 위장관 출혈. 전체 GI 출혈의 약 20~25%. 대부분 원인은 대장(colon)에서 기인하고, Treitz~회맹판 사이 소장 출혈은 따로 small bowel bleeding으로 구분.
기초의학 보강
해부학 기준: Treitz 인대(교과서/Harrison 기준)를 경계로 상부=UGIB / 하부=LGIB. 임상 가이드라인은 내시경 도달 범위를 반영해 IC valve(회맹판)를 기준으로 삼음 — 위내시경은 duodenum 2nd portion까지, 대장내시경은 IC valve 상방 terminal ileum ~10cm까지 관찰하기 때문.
hematocheziamelenaoccult bloodclinical presentation
혈변(Hematochezia): 신선한 적색혈, LGIB의 전형적 양상. 대량 상부출혈에서도 발생 가능 → 혈역학적 불안정 동반 시 UGIB 의심·즉각 평가. 흑색변(Melena): tarry·black·악취변, 혈액이 장내 ≥14시간(3~5일) 체류, 근위부 출혈일수록 흔함, 소장출혈에서도 가능 → 상부 GI 출혈 배제 필요. 잠혈(Occult): 변색 없음, 45~50세부터 대장암 선별(FOBT/FIT), 양성 → colonoscopy, right colon 병변·철결핍성빈혈(IDA) 동반.
hemodynamicspostural hypotensiontransfusion thresholdHb 7g/dL
초기평가에서 심박수·혈압이 가장 중요한 지표. Postural tachycardia/hypotension → 유의미한 출혈. Tachycardia → 대량출혈 진행중. Recumbent(앙와위) hypotension → 가장 중증(보통 기립성 변화가 먼저). 수혈: Hb <7 g/dL, 제한적 수혈전략(7 vs 9)이 재출혈·사망 ↓ (대규모 RCT).
기초의학 보강
기립성 변화(누웠다 일어날 때 HR↑/BP↓)는 순환혈액량 감소를 재현성 있게 반영 → 출혈량 추정 지표. 제한적 수혈전략의 근거: liberal(9) 대비 restrictive(7)에서 재출혈·사망률이 더 낮음.
hemodynamicstachycardiarecumbent hypotensionresuscitation
"Hemoglobin may be normal or only minimally decreased at initial presentation of a severe bleeding episode." Whole blood 출혈 → Hb 즉각 감소 X. Extravascular fluid shift가 일어나야 Hb 감소(최대 72시간, 보통 4~8시간). 저혈압·빈맥에도 Hb 정상일 수 있어 대량출혈 배제 불가. 만성출혈은 정상 혈압에도 Hb 매우 낮을 수 있음. IDA: low MCV, high RDW.
Oakland scorerisk stratificationsafe dischargeESGE BSG guideline
병력(동반질환·복용약) → possible etiology. V/S·P/Ex·DRE·lab → severity. Oakland score: LGIB 중증도 지표. Score ≤8 → 95% 확률로 safe discharge, 외부 validation 완료, ESGE·BSG 강력 권고.
Oakland scorerisk stratificationDRE findingsheart rate
Oakland score 구성 변수: 나이, 성별, 이전 LGIB 입원력, DRE 소견(혈변 유무), 심박수(HR), 수축기혈압(SBP), Hemoglobin. 각 항목 점수 합산 → ≤8점이면 safe discharge 가능.
LGIB algorithmhemodynamic instabilityflexible sigmoidoscopymanagement flowchart
혈역학적으로 unstable한 hematochezia 환자에서 첫 단계 = Upper GI bleeding을 rule out(위내시경). UGIB 배제 후 → bowel prep 후 colonoscopy, colonoscopy 불가/위급 시 → angiography 고려.
교수 강조"이 알고리즘 표는 족보 중의 족보 — 몇 년이 지나도 바뀌지 않는다." 시작은 항상 UGIB r/o.
upper GI sourceBUN/Cr ratioPUD historyUGIB differentiation
심한 hematochezia 환자의 ~15%는 상부 출혈원. UGIB 시사 소견: BUN/Cr >30~35(specificity 90%), BUN >21 mg/dL(specificity 93%), PUD·간질환 병력, aspirin/NSAID 사용, L-tube irrigation(+). L-tube irrigation: 민감도 낮음(28%), NPV <1% — 음성이어도 UGIB 배제 불가. 혈역학적 불안정 동반 hematochezia → 강하게 의심되면 upper endoscopy로 근위부 출혈원 배제.
기초의학 보강
장내 혈액의 단백질이 소화·흡수되어 요소(urea)로 전환 → BUN 상승, BUN/Cr ratio 증가. 이것이 상부출혈을 시사하는 기전.
page10
기출 — 혈변+혈역학적 불안정 응급 평가 (25-58 외)
기출문제hematocheziahemorrhagic shockemergency evaluation
다량 혈변 + 혈역학적 불안정 환자의 응급 초기 평가/접근. 혈역학 평가(HR·BP) → 수액 소생 → unstable hematochezia는 UGIB r/o(상부내시경) 우선.
기출 2025-58 · 2023-68 · 2022-20
다량 혈변과 혈역학적 불안정을 보이는 환자의 응급 평가·접근(정답 1/1/3)
정답·해설 보기
정답: 1 / 1 / 3
직관 unstable + hematochezia → 혈역학 안정화 + UGIB 배제가 핵심.
hematocheziadizzinessGI bleeding
어지러움 + 선혈변 → 유의미한 출혈. 혈역학 평가 + 수액/수혈 + 출혈원 평가 순.
기출 2022-49 · 2021-41 · 2019-41
어지러움+선혈변 환자 GI 출혈 초기 평가(정답 4/2/1)
정답·해설 보기
정답: 4 / 2 / 1
직관 postural 증상=유의미한 출혈량 → 즉각 평가.
hematocheziamelenaabdominal pain
선혈변+흑색변+복통 → 출혈원 감별. Melena 동반 시 상부/근위부 출혈 고려.
기출 2020-10 · 2018-36
선혈변·흑색변·복통 환자 출혈원 감별(정답 4/4)
정답·해설 보기
정답: 4 / 4
직관 melena=체류시간↑(근위부) 감별 단서.
melenaGI bleedingupper source
흑색변 → 상부 GI 출혈을 먼저 고려. BUN/Cr, 병력(PUD·NSAID)으로 상부 시사.
기출 2023-2학기-8 · 2022-1학기-25 · 2021-1학기-25
흑색변 환자 상부 vs 하부 GI 출혈 접근(정답 1/3/1)
정답·해설 보기
정답: 1 / 3 / 1
직관 melena 단독=상부 우선 r/o.
melenadizzinessDRE
어지러움+흑색변 → 혈역학 평가 + DRE로 변양상 확인 → 상부출혈 배제.
기출 2021-1학기-38 · 2021-2학기-15 · 2021-2학기-27
어지러움+흑색변 환자 DRE 포함 초기 평가(정답 3/1/1)
정답·해설 보기
정답: 3 / 1 / 1
직관 DRE로 변색·잠혈 즉시 확인.
hematocheziadyspepsiasmoking history
선홍색 혈변 + 속쓰림 + 흡연력 → 상부 출혈원(PUD) 가능성 감별. 흡연·NSAID는 UGIB 위험인자.
기출 2021-2학기-34 · 2020-2학기-25
선홍색 혈변+속쓰림+흡연 환자 출혈원 감별(정답 4/2)
정답·해설 보기
정답: 4 / 2
직관 속쓰림+흡연=PUD 시사, 선혈변도 massive 상부 가능.
page16
LGIB 알고리즘 재확인 (진단검사 도입)
진단LGIB algorithmhemodynamic instabilityflexible sigmoidoscopydiagnostic flowchart
UGIB rule out 후 → 가급적 bowel preparation 후 colonoscopy. Colonoscopy 불가/위급(bowel prep 어려움) → angiography 고려.
colonoscopyoral lavage prepurgent vs electivediagnostic therapeutic
Colonoscopy: 입원 LGIB의 standard approach, oral lavage 장정결 후 시행, 진단+치료 동시 가능. Urgent(24h) vs Elective(>24h) — urgent는 select high-risk(예: PPB)에만. Flexible sigmoidoscopy: 주로 <40세, minor rectal bleeding에만 적절, CRC 가족력·IDA 있으면 full colonoscopy 고려.
colonoscopyurgent colonoscopyendoscopic hemostasisrebleeding
ACG 가이드라인: 입원 LGIB 환자에 emergent colonoscopy는 불필요 — 24시간 내 급히 할 필요 없음. 장정결로 시야 확보 후 시행이 outcome에 유리.
colonoscopyendoscopic therapystigmata of recent hemorrhageoutcome
Urgent colonoscopy 적응증: 원인·위치가 분명한 경우(예: post-polypectomy bleeding), 지속 출혈로 organ failure 위험인 high-risk 환자. Full colonoscopy 필수: IDA 또는 CRC 개인/가족력의 high-risk 군(proximal colon까지 평가). Sigmoidoscopy는 optional(40세 미만·minor rectal bleeding).
page20
기출 — 변비+체중감소+혈변 검사 선택 (2020-1 8 외)
기출문제constipationweight losshematocheziacolonoscopy work-up
변비+체중감소+혈변 → 대장암 의심 → 검사 선택 = 대장내시경(전대장).
기출 2021-6 · 2020-8 · 2019-4
변비+체중감소+혈변 환자 적절한 검사 선택(정답 5/5/4)
정답·해설 보기
정답: 5 / 5 / 4
직관 alarm feature(체중감소)+혈변 → full colonoscopy.
hematocheziaweight losscolorectal cancer suspicion
혈변+체중감소 → 대장암 의심 work-up. full colonoscopy + 조직검사.
기출 2020-2학기-41 · 2023-1학기-6 · 2022-1학기-6
혈변+체중감소 대장암 의심 work-up(정답 3/3/3)
정답·해설 보기
정답: 3 / 3 / 3
직관 alarm sx → 종양 r/o이 우선.
page22
LGIB 영상검사 — RBC scan·CT/angiography
검사/영상99mTc-labeled RBC scanscintigraphyangiographyminimal bleeding detection
99mTc-labeled RBC scan: minimal bleeding 검출, 최대 24h 반복영상, scintigraphy 양성 → urgent angiography. 국소화 정확도 낮음 — 실제로는 거의 안 함. CT angiography(점점 선호): gut 내 조영제 누출(extravasation) 검출. Massive LGIB + 지속 불안정 + hematochezia → colonoscopy/scintigraphy 시도 없이 urgent angiography. 단, 너무 massive가 아니면 angiography 전 CTA 먼저 권장.
기초의학 보강
표지(99mTc)된 적혈구가 출혈 부위로 누출되는 것을 감마카메라로 검출 → 미량 출혈에도 민감. 단 위치 정밀도는 낮아 후속 angiography 필요.
second-look endoscopyvideo capsule endoscopyobscure GI bleedingsmall intestine evaluation
1. Second-look endoscopy(상부+대장 재시행, ~25% 발견). 2. Video Capsule Endoscopy(VCE) — 표준 다음 단계(yield 56%), 전체 소장 평가, 한계: 조직검사·치료 불가, 시야 불완전, stricture 의심 시 retention 위험 → CT enterography 먼저. 3. CT enterography: VCE 음성 후, 소장 종괴 민감도 높음. 4. Device-Assisted Enteroscopy(DAE): double/single-balloon·spiral, 검사+조직검사+치료 가능, VCE 양성 후 most common 다음 단계. 모두 음성+지속출혈 → intraoperative endoscopy.
page24
기출 — Capsule endoscopy 특징 (22-5 외)
기출문제capsule endoscopysmall bowel imagingnon-invasive
Video capsule endoscopy 특징: 비침습적, 전체 소장 관찰 가능. 단점: 조직검사·치료 불가.
기출 2022-1학기-5 · 2021-2학기-20
캡슐내시경의 특징으로 옳은 것(비침습·소장 관찰)(정답 2/2)
정답·해설 보기
정답: 2 / 2
직관 VCE=비침습·소장 전체·but 인터벤션 불가.
page25
대장 출혈 원인 개요 (빈도순)
목차/개요colonic bleeding sourceshemorrhoidsdiverticulosisangiodysplasiafrequency ranking
치핵·항문질환(30~40%): LGIB 최다 원인, 대부분 경미, 항문통증 동반, 보존적 치료. 대장게실(~20%): hemorrhoid 제외 시 m/c, acute·painless. 혈관이형성증(~10%): age>70, proximal colon, Heyde syndrome(vascular ectasia + aortic stenosis), chronic·intermittent, 혈역학적 의미는 드묾. 기타(~20%): neoplasm, ischemic colitis, IBD, NSAIDs, radiation proctitis, post-polypectomy, SRUS, varices(m/c rectal).
교수 강조"치핵을 제외하면 가장 흔한 원인은 게실(diverticulosis)." 임상적으로 의미있는 LGIB는 치핵 제외하고 보므로 실질 최다 = 대장게실.
hemorrhoidsrectal ulcerbright red bloodanal disease
소량의 선홍색혈(bright red blood)이 전형적, 때로 임상적으로 의미있는 출혈도 발생. Hemorrhoids → LGIB 입원의 10%. Rectal ulcer → LGIB의 최대 8%, 주로 고령·쇠약·변비 환자.
page27
게실 출혈 (Diverticular Bleeding) — 임상양상
임상양상diverticular bleedingpainless bleedingright colon diverticulaabrupt onset
Abrupt onset, painless, 때로 massive bleeding. 80%는 right colon 게실에서 기원(게실 자체는 left side가 더 흔하지만). Chronic/occult bleeding은 비전형적. 자발지혈 ≥90%(US/유럽). 재출혈 ~15%/4~5년(서양; 아시아는 더 높음).
기초의학 보강
우측 게실에서 출혈이 많은 이유: 우측 결장 게실은 목(neck) 부위 vasa recta가 더 노출·취약 → 무통성 다량 동맥성 출혈.
diverticular bleedingspontaneous hemostasisclinical features
Diverticular bleeding 특징: 무통성·갑작스런·대량, 대부분 자발 지혈.
기출 2022-52 · 2025-1학기-2 · 2023-1학기-3
게실 출혈의 특징으로 옳은 것(자발지혈·무통성)(정답 2/4/1)
정답·해설 보기
정답: 2 / 4 / 1
직관 painless+massive+spontaneous cessation이 key.
page29
게실 출혈 — 역학 (natural course)
역학diverticulosisage prevalencediverticular bleeding ratespontaneous cessation
Diverticulosis가 있다고 다 합병증이 오는 것은 아님. 20~25%에서 합병증(실제 5~10%): diverticulitis 10~25%, bleeding ~10%(10년 추적), 그중 재출혈 ~20%.
diverticulosis locationdiverticulitis locationleft vs right colonepidemiology
서양: 출혈은 right side, 게실 자체는 left side가 많음. 아시아: 게실이 양측에 흔함 → 출혈도 right만이 아니라 left side에서도 흔함.
diverticular bleedingvasa rectadiverticulum structurebleeding mechanism
게실의 out-pouching sac 목 부위 vasa recta 파열로 출혈. 내시경: 작은 게실 입구에서 혈성 분비가 "샘솟듯" 나옴. 들어가면 멈춰있고 다량의 변+혈액이 고여있는 경우 많아 출혈점 찾기 어려움(포지션 변경으로 발견). 치료: indirect clipping(입구를 다수 clip으로 봉합).
기초의학 보강
게실은 점막 약화부(weak portion)가 out-pouching → 그 경부의 vasa recta(직혈관)가 노출·파열되어 동맥성 출혈. 무통성·다량의 기전.
diverticulum structureout-pouching sacbleeding vesselschematic illustration
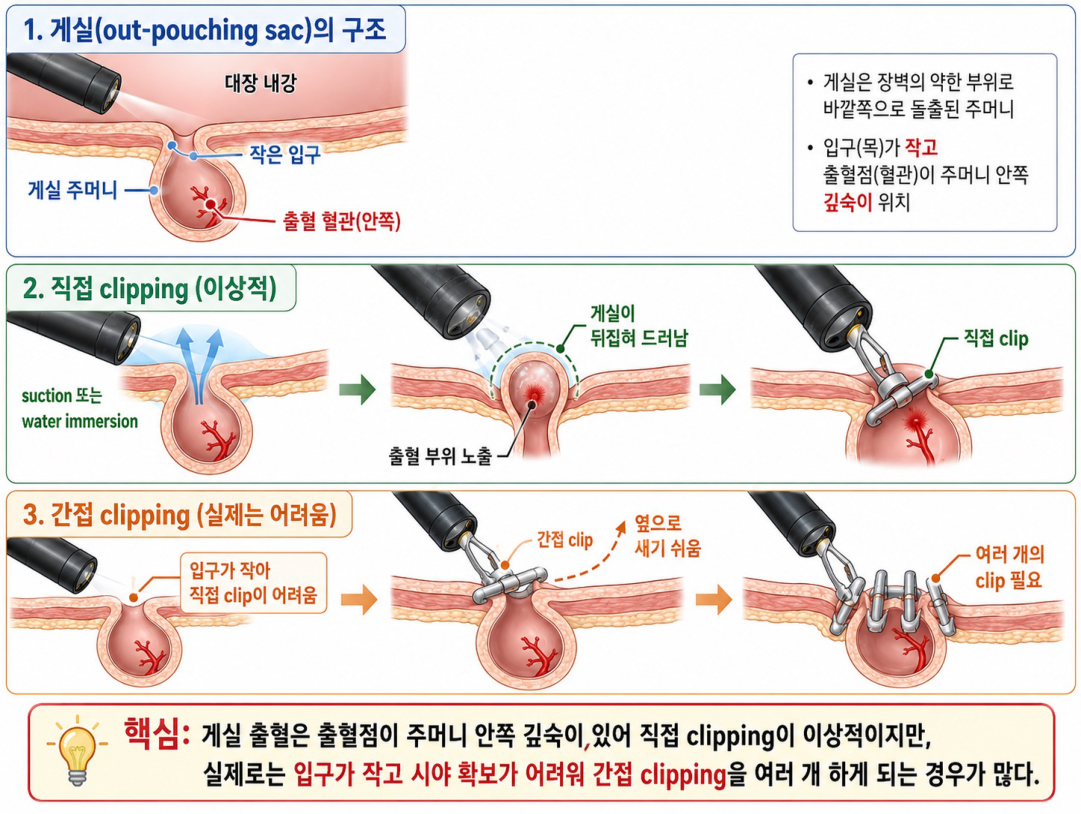
모식도: ① out-pouching sac 구조 — 점막이 바깥으로 주머니처럼 돌출. ② direct clipping(이상적) — sac을 suction/water immersion으로 드러낸 뒤 경부를 직접 clip(권고이나 구멍이 작아 실제 어려움). ③ indirect clipping(현실) — 입구를 가로질러 여러 clip으로 봉합.
page33
게실 출혈 — 단계적 치료 (Stepwise)
치료diverticular bleeding managementendoscopic hemocliptranscatheter arterial embolizationstepwise treatment
Step 1 — 내시경적 지혈: 출혈 게실 확인 시 hemoclip(primary)·coil·APC (EBL/coagulation은 perforation 위험으로 잘 안 함). Step 2 — Superselective TAE(경도자 동맥색전술): angiography에서 출혈 확인 시, 대부분 지혈 성공. Step 3 — Segmental surgical resection: 지속·불응성 출혈(proximal은 right hemicolectomy) — 최후 수단.
page34
기출 — 게실 출혈 내시경 지혈 (본2-1 42 외)
기출문제diverticular bleedinghematocheziaendoscopic hemostasis
Hematochezia로 내원한 게실 출혈 → 내시경적 지혈(hemoclip)이 1차.
기출 2023-69 · 2022-51 · 2020-28
게실 출혈 환자의 적절한 처치(내시경 지혈)(정답 1/4/3)
정답·해설 보기
정답: 1 / 4 / 3
직관 출혈 게실 확인 시 1차=clip.
diverticular bleedingrebleedingendoscopic therapy
내시경 지혈 후 재출혈 → 단계 상향: superselective TAE, 불응 시 segmental resection.
기출 2019-42 · 2018-37 · 2021-1학기-27
게실 출혈 내시경 지혈 후 재출혈 시 처치(정답 5/1/1)
정답·해설 보기
정답: 5 / 1 / 1
직관 재출혈=Step 상향(TAE).
page36
혈관이형성증 (Angiodysplasia / Vascular ectasia)
임상양상angiodysplasiavascular ectasiacecum ascending colonpainless bleeding
상·하부 위장관 전체에 발생, cecum·ascending colon이 m/c. Painless bleeding(occult·melena·hematochezia), LGIB의 4%. 소견: flat·red lesion(2~10mm), 중심 혈관에서 방사상으로 뻗는 ectatic peripheral vessel("거미줄"). 고령·CKD(투석) 환자. 젊은 환자는 보통 소장 기원.
page37
종양 (Neoplasm — Polyps and carcinoma)
임상양상neoplasmcolorectal carcinomapolypsoccult blood loss
양성 용종·암 → 만성 잠혈성 출혈 또는 간헐적 anorectal hematochezia. Acute LGIB의 최대 7%. 대량보다는 간헐적·소량 또는 IDA 형태로 발현.
page38
용종절제 후 출혈 (Post-polypectomy bleeding)
병인post-polypectomy bleedingdelayed bleedingpolypectomy complication
Post-polypectomy / post-EMR bleeding: 요즘 실제 흔한 원인. EMR로 절제한 부위의 노출된 submucosal vessel에서 출혈 — 즉각 또는 지연성(delayed)으로 발생. submucosal injection이 가라앉으며 기존 혈관 노출 → 출혈.
page39
염증성 장질환·장 베체트 (IBD / Intestinal Behcet)
임상양상inflammatory bowel diseaseulcerative colitisCrohn's diseaseintestinal Behcet
IBD(특히 ulcerative colitis): 출혈은 occult ~ 반복적 hematochezia(보통 변에 혼합). 동반: 복통·tenesmus·urgency. Crohn보다 UC에서 prominent. Intestinal Behcet도 감별.
page40
방사선 직장염 (Radiation proctitis)
임상양상radiation proctitisrectal telangiectasiaanorectal bleedingpost-pelvic radiation
골반강 방사선치료(전립선암·방광암·자궁경부암 등) 후 수개월~수년 뒤 발생하는 anorectal bleeding. 소견: multiple rectal telangiectasia(거미줄 모양), 건드리지 않아도 출혈. 치료: argon plasma coagulation(APC)으로 표재 혈관 소작.
page41
기출 — 무통성 선혈변 Angiodysplasia (23-70 외)
기출문제painless hematocheziaangiodysplasia
무통성 선혈변 + 고령/CKD → Angiodysplasia 시사. cecum/ascending colon 호발, 치료 APC.
기출 2023-70 · 2022-1학기-4 · 2021-1학기-11
무통성 선혈변 환자 angiodysplasia 진단/처치(정답 2/3/3)
정답·해설 보기
정답: 2 / 3 / 3
직관 painless+고령/CKD+우측대장 → angiodysplasia.
radiation proctitisprostate cancerandrogen deprivation therapy
전립선암 골반 RT 후 혈변 → Radiation proctitis. rectal telangiectasia, 치료 APC.
기출 2020-2학기-16
전립선암 방사선치료 후 발생한 혈변의 진단(radiation proctitis)(정답 3)
정답·해설 보기
정답: 3
직관 골반 RT 병력+직장 telangiectasia가 결정적.
page43
소장 출혈 — Vascular ectasia·종양·NSAID (1/2)
임상양상small bowel bleedingvascular ectasiaangiodysplasiarebleeding
Obscure bleeding의 ~75~80%는 소장 기원. Vascular ectasia(angiodysplasia): 성인 소장 출혈 m/c, 재출혈 매우 흔함(45%/26개월). 치료: 내시경 지혈(초기 효과); 약물 — estrogen/progesterone 효과 없음, octreotide(case series), thalidomide(1 RCT에서 유의한 효과). Neoplasm: GIST·carcinoid(NET)·adenocarcinoma·lymphoma·전이 — 대개 수술 절제, 영상(CT/MR enterography)으로 확인.
angiodysplasiaendoscopic therapysmall bowel bleedingmanagement
NSAID-induced erosion & ulcer: 성인 소장 출혈 흔한 원인, 소장 전반 발생, VCE로 진단, NSAID 중단이 가장 중요, 원인약 확인·검토. 기타 소장 출혈원: Meckel 게실(소아 m/c, 연령↑하며 빈도↓), Crohn, 감염·허혈·혈관염, 소장 정맥류·게실·duplication cyst, Dieulafoy lesion, aortoenteric fistula. "Obscure GIB의 75%는 소장 기원으로 추정".
page45
Meckel 게실 — 임상양상·진단 (rule of 2s)
임상양상Meckel diverticulumrule of 2sectopic gastric mucosapainless hematochezia
증례: M/17, 첫 hematochezia, painless. 양측 내시경·CT 음성(소장 collapse로 안 보임) → VCE에서 mass 양상 + double lumen sign → entero-CT에서 회장 게실 확인 → 절제 확진. rule of 2s: 인구의 2%, IC valve 상방 2 feet, 길이 2 inches, 흔한 이소성 조직 2종(위·췌장), 호발연령 2세, 남:녀 2:1.
기초의학 보강
Meckel 게실의 이소성 위점막(ectopic gastric mucosa)이 위산을 분비 → 인접 회장 점막에 궤양 형성 → 무통성 출혈. (다음 페이지 Meckel scan의 원리와 연결).
Meckel diverticulumMeckel scan99mTc-pertechnetateectopic tissue
Meckel scan: 99mTc-pertechnetate가 이소성 위점막(gastric mucosa)에 친화적으로 섭취되어 게실 위치를 영상화. 원인불명 소장출혈·젊은 연령에서 Meckel 의심 시 유용.
기초의학 보강
Pertechnetate는 위점막 점액세포에 섭취됨 → Meckel 게실 내 이소성 위점막이 있으면 우하복부에 비정상 섭취 → 진단. 이소성 위점막의 산분비가 출혈 원인이자 영상 표적.
page47
장 허혈 — 개요 및 분류 (Intestinal Vascular Disease)
정의/총론intestinal ischemiasplanchnic perfusionwatershed areaGriffiths point
Splanchnic perfusion이 장의 대사 요구를 충족하지 못함. 3분류: ① Ischemic colitis — 대장 점막 허혈, 보통 일과성·비폐색성(nonocclusive). ② Chronic mesenteric ischemia — 식후 hyperemia 실패 → intestinal angina. ③ Acute mesenteric ischemia — 혈류 급성 소실 → high-mortality 응급(사망률 ~50%).
기초의학 보강
SMA·IMA의 기시·공급 영역을 알면 허혈 호발 부위(watershed area) 예측 가능. Demand는 있는데 perfusion이 못 따라가 발생.
ischemic colitiswatershed areasplenic flexurerectosigmoidatherosclerosis
주로 고령·죽상경화 환자, 대부분 일과성·비폐색성 허혈. 호발 watershed area: splenic flexure(Griffiths point)·rectosigmoid. 직장은 비교적 sparing(IMA + hypogastric artery 이중 혈류 공급). AAA/ileo-aortic 수술 후 5%에서 발생. 젊은 환자: vasculitis·응고장애·estrogen·장거리 달리기. 증상: hematochezia/혈성설사 + 경한 cramp 복통, 대부분 경하고 self-limited.
기초의학 보강
SMA↔IMA 경계(splenic flexure)와 IMA↔hypogastric 경계(rectosigmoid)는 측부순환 의존 분수계 → 저관류 시 가장 먼저 허혈. 직장은 이중 공급으로 보존됨.
page49
기출 — 고령 혈변 Ischemic colitis (25-57 외)
기출문제ischemic colitishematocheziaelderly
고령 + 혈변(+복통) → Ischemic colitis. watershed area, self-limited 경향.
기출 2025-57 · 2023-66
고령 환자의 혈변 — 허혈성 대장염 진단(정답 3/3)
정답·해설 보기
정답: 3 / 3
직관 고령+복통 동반 혈변 → ischemic colitis 우선.
ischemic colitissevere abdominal painhematocheziacolonoscopy findings
심한 복통 + 혈변 + 대장내시경 소견 → Ischemic colitis(점막 허혈·단절성 병변).
기출 2023-67 · 2022-50 · 2021-40
심한 복통+혈변, 대장내시경 소견으로 진단(정답 3/1/3)
정답·해설 보기
정답: 3 / 1 / 3
직관 watershed 분절의 점막 허혈 소견이 단서.
ischemic colitissigmoidoscopyabdominal X-ray
복통+혈변 → S상결장경 / 복부 단순촬영(thumbprinting)으로 허혈성 대장염 확인.
기출 2021-42 · 2020-9 · 2019-40
복통+혈변 환자 진단검사(S상결장경/복부 X선)(정답 1/3/5)
정답·해설 보기
정답: 1 / 3 / 5
직관 thumbprinting·점막부종 = 허혈성 대장염.
ischemic colitisrecurrent hematochezialower abdominal pain
고령 + 반복 혈변 + 하복부 통증 → Ischemic colitis.
기출 2018-35 · 2023-1학기-22 · 2023-1학기-23
고령 반복 혈변+하복부통 — 허혈성 대장염(정답 5/3/4)
정답·해설 보기
정답: 5 / 3 / 4
직관 고령+하복부통+혈변 반복 패턴.
ischemic colitisatrial fibrillationleft lower quadrant painembolic
심방세동(AF) + 좌하복부통 + 혈변 → 색전성 장허혈 고려(AMI 감별 중요). AF=색전원.
기출 2022-2학기-36 · 2021-2학기-29 · 2022-1학기-23
심방세동+좌하복부통+혈변 — 색전성 허혈(정답 4/5/4)
정답·해설 보기
정답: 4 / 5 / 4
직관 AF=embolic source → SMA 색전(AMI)도 감별.
ischemic colitispostprandial painsigmoidoscopy
식후 복통 + 혈변 + S상결장경 → 허혈성 대장염(또는 만성 장간막 허혈 감별).
기출 2021-1학기-10 · 2020-1학기-31
식후 복통+혈변 환자 진단(정답 4/1)
정답·해설 보기
정답: 4 / 1
직관 식후 통증=장간막 허혈 단서, 혈변+S상경=허혈성 대장염.
page55
허혈성 대장염 — 내시경/영상 소견
검사/영상ischemic colitiscolonoscopy findingsmucosal ischemiaendoscopic appearance

중증도별 내시경 소견 스펙트럼: ① friability 동반 표재성 shallow ulceration → 저절로 호전. ② transmural까지 깊은 ulceration. ③ necrosis(회복 불가) → 수술(절제/stoma) 후 수개월 회복 대기.
page56
만성 장간막 허혈 (CMI) — Intestinal Angina
임상양상chronic mesenteric ischemiapostprandial painSMA occlusionintestinal angina
식후 장 hyperemia가 부적절할 때 발생, 대개 SMA(±celiac) 죽상경화성 폐색. 증상: 식후 상복부/배꼽 주위 통증(식후 30~60분 시작, 1~3시간 지속), 식사 공포(fear of eating) → 진행성 체중감소, 만성 설사 가능.
기초의학 보강
식후 장은 혈류 요구가 증가(소화 hyperemia)하나 SMA 협착으로 공급이 못 따라감 → 수요-공급 불균형 = "intestinal angina"(심근 협심증과 동일 원리, 식사=부하검사).
chronic mesenteric ischemiaduplex ultrasoundCT/MR angiographySMA peak velocity
진단: Duplex ultrasound(SMA peak systolic velocity 상승), CT/MR angiography로 협착 확인. 치료: 혈관재개통 — 혈관내(stent) 또는 외과적 revascularization.
page58
급성 장간막 허혈 (AMI) — 정의·병인
병인acute mesenteric ischemiaarterial embolusSMAatrial fibrillationhigh mortality
혈류의 급성 소실 → 장 허혈/경색. 가장 흔한 원인 arterial embolus(주로 SMA), 흔한 색전원 = 심방세동(AF). 매우 높은 사망률의 응급. 전형: 진찰소견에 비해 심한 복통(pain out of proportion).
기초의학 보강
AF에서 좌심방 혈전 → 색전이 SMA로 이동·폐색 → 급성 장 허혈. SMA가 대동맥에서 예각으로 분지해 색전이 잘 걸림.
acute mesenteric ischemiaembolectomyischemia classificationmanagement overview
치료: 원인별 — 색전성은 embolectomy(색전제거술), 혈전성/비폐색성은 각각 다른 접근. 혈역학 안정화 + 광범위 항생제 + 항응고, 괴사 장은 절제. 조기 진단·재관류가 생존의 핵심.
교수 강조SMA 색전 → embolectomy. 늦으면 장 괴사로 절제. 신속한 revascularization이 관건.
acute mesenteric ischemiamanagement tablearterio-occlusivetreatment of underlying condition
AMI 관리 요약 표(원본): 병인별(arterio-occlusive embolic/thrombotic, nonocclusive) 분류에 따른 처치 — 기저질환 치료, 재관류(embolectomy/thrombolysis/혈관재건), 괴사 장 절제, 지지치료.
page61
마무리
참고closingacknowledgement
하부위장관 출혈(임상양상·초기평가·진단검사·원인별 각론) → 소장 출혈 → 장 허혈(허혈성 대장염·CMI·AMI)까지 정리. 변양상·vital·통증 유무·동반증상으로 감별하는 임상적 접근이 핵심.